

If you want to live a long life, move to this state
+ "Should I use an estradiol patch for night sweats?" A pharmacist in perimenopause weighs in






If you want to live a long life, move to the Aloha state
Unless you dislike sunshine, who wouldn’t want to live in Hawaii? Too bad the average home sale price is $973,555 and a gallon of milk costs like $9 there.
According to a study by MoneyGeek, the state Americans choose to live in shapes how long and well they’ll live. The study looked at healthcare across the U.S., with one of the variables being the average life expectancy.
Hawaii consistently leads in life expectancy, often followed by Massachusetts, Connecticut, New Jersey, New York, Minnesota, and California, though exact rankings vary slightly by data source and year, with Southern states generally having lower life expectancies.
Recent data from the CDC for 2021 shows Hawaii at 79.9 years, Massachusetts at 79.6 years, and Connecticut at 79.2.
Where do Americans live the longest?
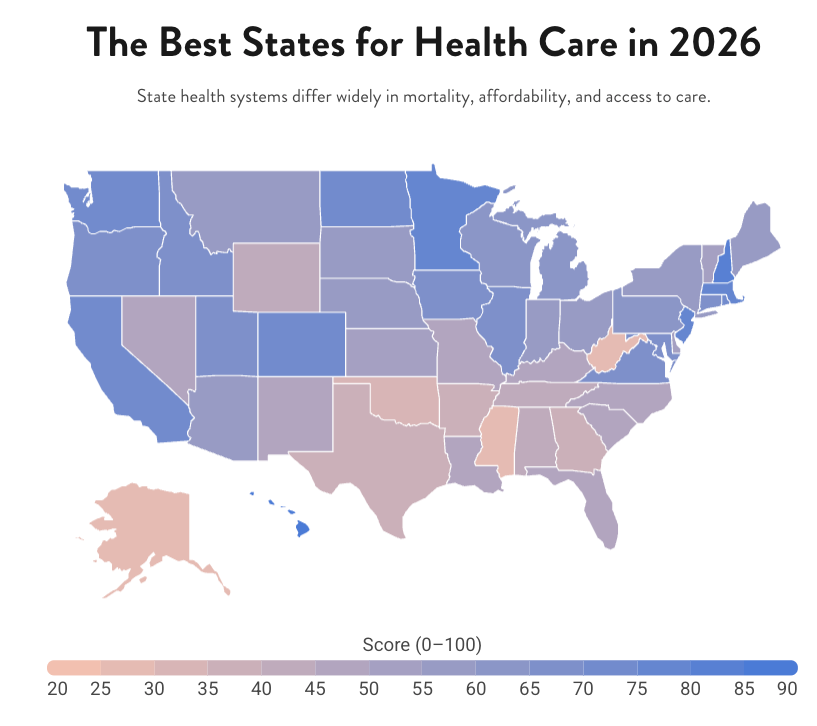
Top 10 states for quality healthcare
Hawaii
New Hampshire (also considered the “healthiest state”)
Massachusetts
District of Columbia
Minnesota (we’re sending you all the love right now)
New Jersey
Washington
Colorado
Rhode Island
North Dakota
These 10 states share several strengths: high insurance coverage, primary care capacity, competitive premiums relative to income, and lower mortality rates.

Should I use the estradiol patch for night sweats?
This is not a story about how an estradiol patch will fix everything. This is about how confusing perimenopause still is and how easy it is to mistake hormonal chaos for a menopausal hormonal decline. This is especially true in a moment when menopause advice is louder, more confident, and more commercial than ever.
When I was the youngest in my group of mom friends, the older women talked about something they called “the change before the change.” It sounded ominous and vague, and I didn’t fully grasp what they meant.
Twenty-some years later, we have a name for that mystery shift: perimenopause. It’s the stretch of years when hormones start behaving unpredictably, often long before periods stop. It can look like waking up at 2 a.m., replaying something that happened yesterday — or decades ago. It can also look like heavier periods. Bigger mood swings. PMS that feels dialed up to eleven. And night sweats that seem to come out of nowhere.
Now I’m 51, with four kids, picking up my fourth grader as the “old mom” at school. I think back to myself at 35, when I first sensed perimenopause looming, and realize I didn’t take my older friends seriously enough. Since then, life has been one long hormonal upheaval: pregnancies, babies, teenagers, and my own steady march through perimenopause. I’m still cycling at 51. It’s still intense.
Even though I knew “the change before the change” could last for years, I still wasn’t prepared for how it would actually feel or what to do about it. And judging by the questions I hear now, many millennial moms entering this phase aren’t either. The difference today is that instead of too little information, there’s too much, especially when so much of it is just marketing dressed up as medical advice.
One of the biggest sources of confusion is what perimenopause actually is. But also: How long does it last? What symptoms count? How do you know when it starts or when it’s over?
What is perimenopause?
Perimenopause is the span of years leading up to natural menopause, when the ovaries begin changing how much estrogen they produce and how regularly they release an egg. Most women enter perimenopause in their mid-40s, though hormonal shifts can begin earlier.
But this sounds a lot simpler than it feels, and so many women are navigating this largely on their own. Recently, a late-30s mom with young kids asked me if hormone therapy might help her night sweats. Would an estrogen patch calm the “meno monster”? Hot flashes mean menopause, right?
Not necessarily.
At what age do women enter perimenopause?
While menopause can occur before 45, it’s pretty uncommon. Around 5% of women enter menopause between 40 and 45, and it’s even less common before 40. And night sweats have many causes that have nothing to do with menopause, or even chronically low estrogen.
In my late 30s, my night sweats were tied to the natural estrogen drop that happens just before a period. The issue wasn’t too little estrogen; it was estrogen volatility. I still had regular cycles, but my hormones were swinging wildly. PMS often worsens after 35, and ovaries can pump out higher peaks of estrogen followed by sharp crashes. Those rapid shifts, not sustained deficiency, can trigger night sweats.
This is why there’s no single blood test that can effectively diagnose perimenopause. Hormone levels fluctuate daily. Testing is usually done to rule out other causes like thyroid issues, anemia, early menopause, or to investigate heavy or painful periods. Clinicians rely on age, symptoms, and cycle patterns, and tracking your periods and symptoms can be far more helpful in understanding the full picture than a snapshot that a lab provides
So back to the night sweats question.
Will the estradiol patch help with night sweats and hot flashes?
If you’re still cycling (in your early perimenopause or late reproductive years), will a menopause estradiol patch help with night sweats or hot flashes?
Sometimes hormone therapy can be prescribed to premenopausal women, but the more important question is whether it will actually help. Menopause hormone therapy (typically referred to as HT or MHT) contains relatively low doses of estrogen, too low to suppress ovulation. If your ovaries are already producing erratic surges of estrogen, adding a small, steady amount may not smooth the ride. In my case, it likely wouldn’t have helped much at all.
That’s why, for women who still cycle and are struggling with symptoms like heavy periods, mood instability, and night sweats, low-dose combination birth control is often prescribed instead. Birth control suppresses ovulation, preventing the hormonal rollercoaster in the first place, and replaces it with a more consistent level of estrogen and progestin. Menopause HT, by contrast, is designed to replace estrogen that the ovaries are no longer making, not to override them when they’re still active.
This isn’t a popular message on social media — or among the many for-profit companies cashing in on the menopause market — but the estrogen patch is not a one-size-fits-all solution. It has an important role for some women with specific symptoms, but years before menopause, fluctuating estrogen, not low estrogen, is often the real issue.
Birth control has another benefit: pregnancy prevention. Contrary to what you may have been led to believe, perimenopause doesn’t mean infertility, and until menopause is confirmed, contraception still matters if you don’t want to get pregnant, even though fertility is less predictable at this stage.
If pregnancy is something you are hoping for, time matters. The late reproductive years can close quickly, and early conversations with a clinician or reproductive endocrinologist can be invaluable.
Whatever path you take, the most important step is finding a clinician you trust, preferably someone who is experienced with this life phase and up-to-date on current research and FDA-approved options. Hormone therapy isn’t mandatory, and it isn’t for everyone. It also requires ongoing conversations, since risks, benefits, and bodies change over time. I’ve found my midwife to be my most helpful guide hormonally, alongside regular care from an internist.
Appointments can feel daunting, but preparing helps. Track your cycle and symptoms. Bring family history when possible. Ask direct questions: What else could be causing these symptoms? What tests make sense? What kind of hormones, at what dose, and why? And don’t forget to discuss fertility goals or contraception.
And after bursting the estrogen-patch miracle bubble, here’s the least exciting truth: all the boring things that have always helped still matter — maybe more after 35. Sleep. Hydration. Whole foods with enough protein, fiber, calcium, and iron. Strength-building movement. Less smoking, alcohol, and late-day caffeine.
None of us does this perfectly. I certainly don’t. One of my biggest health goals now is less perfection, more pleasure. Mental health is health and it’s often the most overlooked part of perimenopause.
Creative outlets, therapy, faith, and real connection have helped me through mood swings and panic attacks. If anxiety, sleep, or mood are disrupting daily life, that’s a reason to seek help, not something to white-knuckle through alone.
Finally — and this should probably come first — find community. Some days you might feel better than ever. Other days you’ll be exhausted and deeply uninterested in “menopositivity.” On those days, being around someone who gets it matters. No wonder creators like @JustBeingMelani resonate so widely.
Community is what pulled me into writing as a second career, starting with my first pitch to The Midst. Amy Cuevas Schroeder didn’t just encourage me to write — she provided the kind of support that turns intention into action.
We’re all on the same path, just at different points. Women supporting women, sharing what we’ve learned, and asking for help when we need it, and that’s a cycle I plan to keep repeating long after my menstrual cycles finally end.
It’s amazing the knowledge you gain being the “old mom.”
This story was originally published here in Meet Me at the Medcart. Learn more about The Midst’s syndication program here; we partner with physicians and health experts to produce and publish their thought leadership about 40+ women’s health and wellness.

Daphne Berryhill is a freelance writer and pharmacist, practicing in oncology infusion and behavioral health pharmacy. Her writing has appeared in GoodRx Health, Forbes Health, the MedShadow Foundation, and The Midst, with additional projects including needs assessments, content strategy, and health outreach for Those Nerdy Girls. She writes two Substack newsletters: Meet Me at the Medcart and Daphne Discloses. She lives near Madison, Wisconsin, with her husband and kids, three at home and one nearby.

“In psychology there’s something called the spotlight effect.
We overestimate how much everyone is watching and judging us.
In reality, we’re far less visible than we think.
Simply put: no one cares.”
 | A guest post by
|
 | A guest post by
|